
Lung blebs are small pockets of air that sometimes develop on the outer layer of your lungs. A lung bleb may sound intimidating but is rarely dangerous and usually easy to treat. However, in some cases, particularly in individuals with conditions like emphysema, large blebs can burst like a balloon, causing a collapsed lung. In this article, we’ll discuss who is at risk for lung blebs, what causes them, and treatment options.
What are Lung Blebs?
Lung blebs are air-filled blisters or cysts that can develop on the lining of the lungs, called the pleura. Often, blebs are asymptomatic, so you can have them without knowing. A person can have just one lung bleb or numerous blebs and might never know they are there unless detected by a CT scan. However, if lung blebs burst, they release air into the chest cavity and can cause the lung to collapse (pneumothorax).
What is the difference between a bleb and a bulla?
A bulla (plural: bullae) is the term used for larger air-filled cavities within the lung tissue that sometimes occur when several blebs are close to each other.
What Is a Pneumothorax?
When lung blebs rupture, the air held in the bleb or bulla escapes into the chest cavity, leading to a collapsed lung, also known as pneumothorax1.
Depending on the degree of collapse and a patient’s overall respiratory status, symptoms can include shortness of breath, difficulty breathing, and chest pain. In larger pneumothoraces or complete lung collapse, a patient may become cyanotic, turning a blue or purplish color, or develop other respiratory distress symptoms2.
What is a Primary Spontaneous Pneumothorax (PSP)?
When patients have no other underlying medical conditions to cause a pneumothorax, doctors call it primary spontaneous pneumothorax (PSP)3. Clinical experience and research have shown that PSP isn’t caused by the simple rupturing of blebs and bullae. Instead, it’s associated with abnormalities spread across both lungs, such as inflammation of the lung lining (pleurisy) or “water on the lungs” (pleural effusion), which is a gathering of fluid between the layers of tissue that line your lungs and your chest cavity4.
Who Is at Risk for Lung Blebs and Bullae?
Certain high-risk occupations could increase your risk of developing lung blebs, such as those that put you in close contact with dust, chemicals, fibers, germs, or smoke, among other things. Blebs and bullae are thought to be tied to an underlying disease such as bronchitis, chronic obstructive pulmonary disease (COPD) such as emphysema, cystic fibrosis, and even cancer. However, even otherwise healthy young people can fall prey to a PSP event, which occur without any underlying disease or injury.
The incidence of PSP in men is 5 to 10 times higher than in women5, while tall, thin people are also more susceptible to PSP, probably due to increased pressure on the top of the lung6.
Are lung blebs hereditary?
About 1 in 10 people who suffer from a PSP have a family member who's also experienced one, and there are some inherited diseases, such as Birt-Hogg-Dubé syndrome, which are associated with lung blebs and PSP. Birt-Hogg-Dubé syndrome is caused by mutations in the FLCN gene, which is inherited from your parents7.
What Causes Lung Blebs and Bullae?
Researchers suspect that tobacco and cannabis smoking, emphysema (also called Chronic obstructive pulmonary disease, or COPD), and other lung conditions can lead to the development of blebs and bullae. That’s because blebs are especially prevalent in damaged lung tissue.
What Causes Lung Blebs to Burst?
Many events can cause blebs to burst, including sudden or deep breaths or changes in air pressure. There is often no clear underlying cause for blebs developing or rupturing.
Types of Lung Bleb and Bulla
Lung blebs are small, typically 1 to 2cm in diameter, while bullae can grow quite large and tend to be between 1 and 20 cm in diameter8. Lung blebs and bullae are often described based on their location within the lung, with the most common being subpleural blebs or subpleural bullae, which are found between the lung lining and the chest cavity. Lung blebs tend to appear in the upper lobes of the lung9, which are referred to as apical subpleural blebs.
Blebs and bullae can also be described based on their association with diseases; for example, emphysematous blebs are associated with emphysema. Emphysema that is characterized by the formation of fluid-filled bullae is called paraseptal lung bullae10.
Diagnosing Lung Blebs and Bullae
Because blebs and bullae are often asymptomatic, you can go through life with many lung blebs and never know. Sometimes, the presence of large bullae is detected by accident when the lungs are being imaged for another reason.
If you show symptoms of emphysema, you should talk to your healthcare provider. These symptoms include:
- Shortness of breath, particularly when exercising
- Persistent coughing
- Tightness in the chest
- Weight loss and swelling in the ankles11
If you have persistent symptoms of emphysema, your doctor might recommend some tests to understand your lung health, including X-rays and computerized tomography (CT) scans, which can reveal the presence of blebs and bullae.
Diagnosing Pneumothorax
The symptoms of a collapsed lung may be mild or severe and include:
- Shortness of breath
- Chest pain, which could be stronger on one side or the other
- Sharp pain when you inhale
- Lung pressure that increases with time
- Lips or skin turning blue
- Increased heart rate
- Rapid breathing
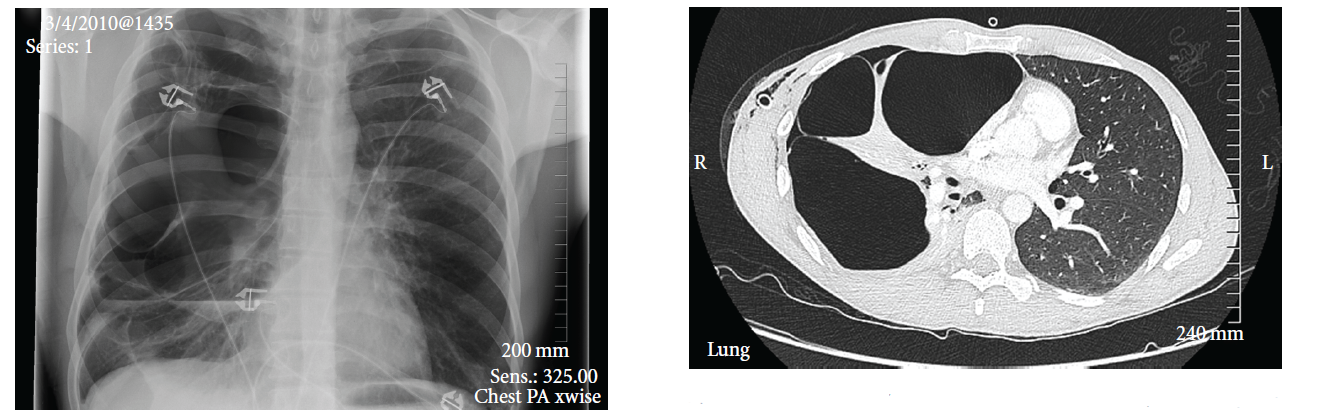
In most pneumothorax cases, a chest X-ray is the first-line diagnostic tool. Doctors may also order an ultrasound to identify pneumothorax. For more detailed images, a CT scan may be necessary.
CT scans use multiple X-rays from different angles and computer-processed combinations to produce high-quality images of the pleural space and any blebs or bullae. Those images can determine the size and location of a bleb or bulla. Technicians may also use computed tomography to help with the placement of a tube thoracostomy.
Lung Bleb Treatment
Lung blebs rarely need surgical intervention. However, in the case of very large bullae, or if you have several instances of pneumothorax, your healthcare provider might recommend a bullectomy - the surgical removal of lung bullae12.
Most surgeons consider video-assisted thoracoscopic surgery (VATS) to be the gold standard in treating pneumothoraces and blebs/bullae13. VATS is a low-intrusion technique that can help with diagnosis and treatment. During a VATS procedure, the surgeon inserts a thoracoscope (chest tube) and surgical instruments into the chest through small incisions in the chest wall. The thoracoscope transmits internal images of the chest to a video monitor to guide the surgeon.
Pneumothorax Treatment
There are several pneumothorax treatment options. However, part of the reason is that some treatments are being debated in the medical community. For instance, while oxygen has been the traditional treatment for small, asymptomatic, or mildly symptomatic pneumothorax, recent medical literature has questioned its effectiveness and recommended further study14.
A tube thoracostomy (chest tube placement) is one of the most common lines of treatment. A chest tube or catheter evacuates air from the thoracic cavity, allowing the lung to heal and re-expand15. The line is removed after a successful water seal trial, preventing air backflow into the pleural space16.
Typically, the first instance of symptomatic PSP is treated through observation and chest tube placement. Your doctor may recommend bleb or bulla resection combined with mechanical pleurodesis — manual scarring of the pleura to prevent the recurrence of spontaneous pneumothorax or pleural effusion — or a pleurectomy, which removes portions of the parietal pleura.
Resection may be indicated for returning patients who have more than one pneumothorax event17. While there’s no real consensus about PSP treatment, clinicians and surgeons tend to treat blebs conservatively because there are still many controversies regarding diagnostic tools and management plans.
A Low-Dose CT Scan (LDCT) Can Help Determine Where Blebs and Bullae Are
Diagnostic imaging, such as a CT scan that reveals blebs or bullae, is also a predictor for surgical intervention since the recurrence risk is progressively higher in patients who have had a previous occurrence of bleb ruptures or pneumothorax. Low-dose computed tomography (LDCT) is the only recommended CT scan for people who are high risk for lung cancer or coronary heart disease.
The National Lung Cancer Screening Trial (NLST) has shown that an LDCT scan reduces lung cancer mortality by 20 percent in high-risk subjects compared to chest X-ray screening18. LDCT screening of heavy smokers is advised19.
Can Lung Blebs Cause Cancer?
There is some evidence that lung blebs and bullae are associated with lung cancer. COPD and emphysema, which are often causes of lung bullae, increase your risk of developing lung cancer20,21. There are some cases of lung cancer developing directly from giant bullae22,23, but no evidence that blebs and bullae in healthy individuals can lead directly to lung cancer.
Preventing Lung Blebs
Lung blebs and bullae occur in healthy individuals and are not normally cause for alarm. While dangerous events like PSP are associated with lung blebs, they are usually treatable in healthy individuals.
However, conditions like emphysema, which are associated with bullae and PSP, are often related to lifestyle factors like smoking. Stopping smoking, eating a balanced diet, and regularly exercising will decrease your chances of developing emphysema and help alleviate your symptoms if you suffer from emphysema.
Summary: Lung Blebs and Their Risks
Lung blebs are usually harmless but can lead to serious complications like pneumothorax. Early detection, lifestyle changes, and medical interventions like VATS can help manage risks. If you experience symptoms, consult a doctor for a proper diagnosis and treatment to protect your lung health.
At Ezra, we know that the best defense against cancer is prevention through early detection. Not only do we offer low-dose CT scanning, we also offer a full-body MRI scan that takes less than an hour and screens your body for abnormalities and potential cancer in up to 13 organs. If you’re at a higher risk for lung bullae, you may want to consider a regular lung screening program.
Understand your risk for cancer with our 5 minute quiz.
Our scan is designed to detect potential cancer early.
References
1. Eckland AK. Blebs, Bullae and Spontaneous Pneumothorax. Thoracic Surgery. February 8, 2012. Accessed April 3, 2025. https://thoracics.org/2012/02/08/blebs-bullae-and-spontaneous-pneumothorax/
2. Medical Definition of Cyanotic. RxList. Accessed April 3, 2025. https://www.rxlist.com/cyanotic/definition.htm
3. Grundy S, Bentley A, Tschopp JM. Primary spontaneous pneumothorax: a diffuse disease of the pleura. Respir Int Rev Thorac Dis. 2012;83(3):185-189. doi:10.1159/000335993
4. Radiology (ACR) RS of NA (RSNA) and AC of. Diffuse Interstitial Lung Disease. Radiologyinfo.org. Accessed April 3, 2025. https://www.radiologyinfo.org/en/info/diffuselung
5. Tsuboshima K, Kurihara M, Yamanaka T, Watanabe K, Matoba Y, Seyama K. Does a gender have something to do with clinical pictures of primary spontaneous pneumothorax? Gen Thorac Cardiovasc Surg. 2020;68(8):741-745. doi:10.1007/s11748-020-01388-1
6. McKnight CL, Burns B. Pneumothorax. In: StatPearls. StatPearls Publishing; 2025. Accessed April 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK441885/
7. Boone PM, Scott RM, Marciniak SJ, Henske EP, Raby BA. The Genetics of Pneumothorax. Am J Respir Crit Care Med. 2019;199(11):1344-1357. doi:10.1164/rccm.201807-1212CI
8. Saxena AK. Treatment of Pulmonary Blebs and Bullae. In: Saxena AK, Höllwarth ME, eds. Essentials of Pediatric Endoscopic Surgery. Springer; 2009:111-115. doi:10.1007/978-3-540-78387-9_15
9. The Lungs and Pleurae | Boundless Anatomy and Physiology | Study Guides. Accessed April 3, 2025. https://www.nursinghero.com/study-guides/boundless-ap/the-lungs-and-pleurae
10. Weerakkody Y. Paraseptal emphysema | Radiology Reference Article | Radiopaedia.org. Radiopaedia. doi:10.53347/rID-17877
11. Emphysema. Accessed April 4, 2025. https://medlineplus.gov/emphysema.html
12. Nakahara K, Nakaoka K, Ohno K, et al. Functional Indications for Bullectomy of Giant Bulla. Ann Thorac Surg. 1983;35(5):480-487. doi:10.1016/S0003-4975(10)60419-5
13. Ng CSH, Lee TW, Wan S, Yim APC. Video assisted thoracic surgery in the management of spontaneous pneumothorax: the current status. Postgrad Med J. 2006;82(965):179-185. doi:10.1136/pgmj.2005.038398
14. Park CB, Moon MH, Jeon HW, et al. Does oxygen therapy increase the resolution rate of primary spontaneous pneumothorax? J Thorac Dis. 2017;9(12):5239-5243. doi:10.21037/jtd.2017.10.149
15. Porcel JM. Chest Tube Drainage of the Pleural Space: A Concise Review for Pulmonologists. Tuberc Respir Dis. 2018;81(2):106-115. doi:10.4046/trd.2017.0107
16. External suction versus simple water-seal on chest drainage following pulmonary surgery: an updated meta-analysis | Interdisciplinary CardioVascular and Thoracic Surgery | Oxford Academic. Accessed April 3, 2025. https://academic.oup.com/icvts/article/28/1/29/5056123?login=false
17. Thoracoscopic Resections and Pleurodesis for Bleb Disease - A SAGES Wiki Article. SAGES. December 5, 2013. Accessed April 3, 2025. https://www.sages.org/wiki/thoracoscopic-resections-and-pleurodesis-for-bleb-disease/
18. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N Engl J Med. 2011;365(5):395-409. doi:10.1056/NEJMoa1102873
19. Wender R, Fontham ETH, Barrera E, et al. American Cancer Society Lung Cancer Screening Guidelines. CA Cancer J Clin. 2013;63(2):107-117. doi:10.3322/caac.21172
20. Stoloff IL, Kanofsky ,Paul, and Magilner L. The Risk of Lung Cancer in Males With Bullous Disease of the Lung. Arch Environ Health Int J. 1971;22(1):163-167. doi:10.1080/00039896.1971.10665827
21. Mouronte-Roibás C, Leiro-Fernández V, Fernández-Villar A, Botana-Rial M, Ramos-Hernández C, Ruano-Ravina A. COPD, emphysema and the onset of lung cancer. A systematic review. Cancer Lett. 2016;382(2):240-244. doi:10.1016/j.canlet.2016.09.002
22. Yoshikawa T, Misao T, Aoe M. Primary lung cancer arising from the wall of a giant bulla in which positron emission tomography was useful for preoperative diagnosis. Gen Thorac Cardiovasc Surg. 2011;59(2):137-140. doi:10.1007/s11748-010-0618-7
23. Ema T. Large cell carcinoma on the bullous wall detected in a specimen from a patient with spontaneous pneumothorax: report of a case. J Thorac Dis. 2014;6(10). doi:10.3978/j.issn.2072-1439.2014.09.29



